
On the evening of April 21, 2026, ThS.BSCKII Nguyễn Văn Lưu and his team at BVDK Tâm Anh in Ho Chi Minh City put a titanium rod down my right femur and held the fracture together with a screw that runs from the lateral cortex up into the head of the femur. The whole operation took roughly an hour of cutting time. This article unpacks exactly what the hardware is and why it was the right choice for this fracture pattern. It is the article I was looking for during the first 48 hours after surgery, when "you have a PFN" did not mean very much to me.
The Fracture
The injury was a comminuted intertrochanteric fracture of the right femur, extending subtrochanterically, with calcar femorale involvement and a lesser-trochanter avulsion fragment. On the AO/OTA classification, the closest match is 31A3: the reverse-oblique intertrochanteric pattern that behaves clinically like a subtrochanteric injury, multifragmentary and unstable, with the medial cortical buttress disrupted. The hospital's discharge code is ICD-10 S72.1 (intertrochanteric); the operative description uses the word "subtrochanteric" because the comminution extends into that region. Both labels describe the same construct.
Three features of the fracture drove the choice of hardware:
- Location is in the highest-stress zone of the skeleton. The subtrochanteric region of the femur experiences the highest bending and compression stresses of any bone in the body during normal gait. Whatever holds this fracture has to carry real load while the bone heals.
- Comminution at the calcar. The medial cortical buttress that normally transfers load from the head to the shaft is fragmented. The natural compressive load path is broken until callus bridges the gap.
- The fragment includes the femoral head. Any reconstruction must capture the proximal fragment (head and neck) and reconnect it to the shaft. That requires a fixation device that crosses the fracture in a way that loads the head correctly.
Together, those three features rule out conservative management, rule out most plate constructs, and point hard at a cephalomedullary intramedullary nail. Which is exactly what went in.
The Implant: Mediox Proximal Femoral Nail
The implant card BVDK Tâm Anh issued at discharge lists the construct in full:
- Implant type: Cephalomedullary intramedullary nail with cephalic lag screw + distal interlock + end cap
- Manufacturer: MEDIOX Orvosi Műszergyártó Kft, 3324 Felsőtárkány, Hungary
- Model: Mediox Proximal Femoral Nail (PFN), right-side, cannulated, 130° cervico-diaphyseal angle
- Material: Ti6Al4V ELI titanium alloy (ASTM F136)
- Implanted: 21/04/2026, ~23:00 ICT, BVDK Tâm Anh, Tân Bình, HCMC
Anatomy of the construct
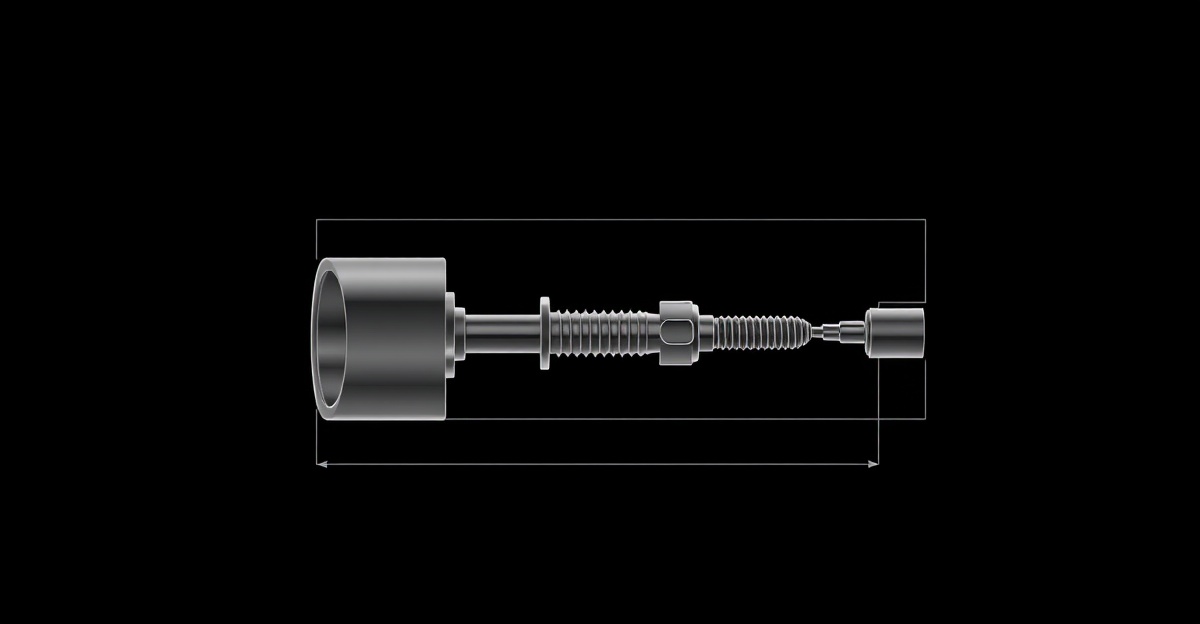
The construct is four discrete pieces of titanium working together:
- The nail. A long, cannulated titanium rod that sits inside the femoral canal. Enters at the greater trochanter and runs down the shaft. The 130° angle at the proximal end is the angle between the nail axis (along the shaft) and the lag-screw axis (up into the femoral neck), chosen to match average native femoral anatomy.
- The cephalic lag screw. A large screw that enters from the lateral cortex, passes through a hole in the side of the nail, and continues up into the femoral neck and head. This is the piece that holds the proximal fragment to the rest of the construct. The screw is offset from the nail's central axis specifically to track the natural neck-shaft angle.
- The distal interlocking screw. A smaller transverse screw that passes through the nail near its distal end, locking the nail rotationally to the femoral shaft. With one distal screw, the construct is "statically locked", which is what you want for early controlled loading. Two distal screws ("dynamically locked") are used in certain shaft fractures where micromotion at the fracture site is desired.
- The end cap. A small threaded cap that seals the proximal end of the cannulated nail, preventing bone ingrowth into the canal that would make removal harder if it were ever needed.
Why this geometry
The 130° cervico-diaphyseal angle approximates the average native angle between the femoral shaft and the femoral neck in an adult. When the lag screw is seated in the femoral head and the nail is centered in the canal, the construct recreates the natural load axis of the proximal femur. Compressive load from the head travels down the lag screw, into the nail, and out into the shaft. That is the same path the calcar would normally take if it were intact.
Cannulated means the nail has a hollow core. This lets the surgeon pass a guide wire down the femoral canal first, confirm position fluoroscopically, and then advance the nail over the wire. Far more predictable than a solid nail in a fracture environment.
The Material: Why Titanium, and Why ELI
Ti6Al4V is the workhorse of orthopaedic implants. It is roughly half the weight of stainless steel, with a Young's modulus much closer to cortical bone than steel. That reduces stress shielding (the phenomenon where a too-stiff implant takes so much load that the surrounding bone weakens). It is corrosion-resistant in physiologic conditions and biocompatible, with no documented allergy in the vast majority of patients.
The "ELI" suffix (Extra Low Interstitial) narrows the specification further. ASTM F136 caps oxygen, nitrogen, and iron content at lower levels than standard Ti6Al4V (ASTM F1472). These trace elements are interstitials in the titanium lattice. Reducing them improves ductility and, more importantly, improves fatigue strength under cyclic loading. An implant in a 94 kg athlete who plans to return to running and Ironman racing benefits directly from that fatigue margin.
Two practical implications fall out of the material:
- MRI is fine within manufacturer-specified conditions. Titanium is paramagnetic, not ferromagnetic. The implant will not move or heat dangerously in a properly conducted MRI at 1.5T or 3T. For imaging of the right femur or hip directly, request MARS (Metal Artefact Reduction Sequences). This minimizes the bloom around the metal so the surrounding tissue can be evaluated.
- Airport security is fine. Declare it. The titanium itself does not trigger metal detectors at the same intensity as steel, but the volume of metal in the construct is enough to flag most modern scanners. A copy of the implant card on the phone, plus a one-line explanation, makes the conversation quick.
Why an IM Nail and Not a Plate
The two real options for surgical fixation of a subtrochanteric femur fracture are an intramedullary nail (mine) and a sliding hip screw with side plate (DHS), or in some cases an angled blade plate or proximal femoral locking plate. Each has its place. For my fracture pattern, the IM nail is biomechanically the stronger construct, for two reasons.
Load path runs through the nail, not off-axis
A laterally placed plate sits on the outside of the femur. Body weight coming down through the femoral head creates a bending moment that the plate resists in cantilever: load enters at the femoral head, bends the construct sideways, and is resisted by the plate working in three-point bending. The implant takes the full load on its own until callus forms.
An IM nail sits in the centre of the canal. The lag screw transfers head load directly into the nail axis. There is no bending moment to fight, only axial and torsional load, distributed along the length of the nail. The implant works in compression and torsion, which is exactly what a titanium rod is good at.
Load sharing as bone heals
With a plate, the bone behind the plate is shielded from load until the plate fails or is removed. The bone in that region remodels weakly, creating a long-term failure risk. With an IM nail, as callus forms and matures, the bone gradually takes more of the load. Same principle as a cast on a child's forearm fracture, scaled up and made of titanium. The implant becomes progressively less load-critical as the bone heals.
The published failure rates and reoperation rates for IM nails in subtrochanteric fractures are consistently lower than for plates in the same anatomic zone. Plates remain the right call when the fracture extends too far distally for the nail to capture both ends, or when severe canal narrowing rules out IM fixation. Neither applied to my fracture, and the IM nail was the correct choice.
The Hardware Is the Limiting Factor
The one sentence my surgeon said that reframed the whole rehab plan: the emergency-stock nails available on the day were not ideally sized for my frame. The bone was reduced anatomically. The implant geometry is correct. But the construct is not the most over-engineered version of itself for a 94 kg, 196 cm muscular patient.
The downstream implication is simple. Every weight-bearing decision for the first six months flows from the hardware, not the bone. The bone will heal at the rate biology allows. Pushing weight bearing before callus bridges the calcar gap loads the construct in three ways that matter:
- Varus collapse. Compressive load on a not-yet-bridged calcar can tilt the proximal fragment medially, changing the neck-shaft angle. Varus deformity shortens the leg and changes hip mechanics for life.
- Lag-screw cut-out. The lag screw can migrate superiorly through the femoral head if loaded before the bone supporting it is strong enough. This is a catastrophic failure requiring revision.
- Implant fatigue. Cyclic loading near the elastic limit of titanium (under-sized for body weight, with the calcar gap still open) accumulates microcracks. Implant breakage is rare but real.
None of these are likely if the protocol is followed. All of them are avoidable. The cost of patience is six weeks on crutches. The cost of pushing is a second operation. That is a one-sided trade.
What the Imaging Showed
Day 0: post-operative AP X-ray (2026-04-22, 10:10 ICT)
Anatomic reduction. Nail centred in the canal. Lag screw seated centrally in the femoral head with appropriate inferior-anterior position (the classic "centre-centre" target, with Tip-Apex Distance well within the 25 mm threshold associated with low cut-out risk). Distal interlocking screw through the nail, statically locked. Neck-shaft angle restored. No visible fracture gap. No varus or valgus malalignment.
Day 15: Week 2 follow-up X-ray (2026-05-06)
Hardware position unchanged from Day 0. No varus collapse. No lag-screw migration. No peri-hardware lucency that would suggest implant loosening or infection. Subtle haziness along the medial cortex near the fracture line, consistent with very early periosteal callus initiation (woven bone, pre-bridging). Fracture line still clearly visible, as expected at two weeks post-op.
Pending: Week 6 follow-up X-ray (2026-06-03)
The decision-gating image. We are looking for bridging callus on the medial cortex: woven bone visible across the fracture line on multiple views. If present, the protocol advances to 25% partial weight-bearing with crutches. If not, weight bearing remains zero for another two to four weeks pending the next imaging.
Hardware in an Endurance Athlete
The clinical literature on intramedullary nails is overwhelmingly written about sedentary or older patients. The implant is the same titanium rod for a 75-year-old hip-fracture patient and a 46-year-old Ironman trainee, but the questions that matter are different. This section covers what changes when the patient plans to run, ride, swim, push sleds, and race long-distance triathlon for at least another decade.
Fatigue life under repeated loading
Titanium has good fatigue resistance, but it is not infinite. Every running stride loads the proximal femur with roughly 2.5 to 3.5 times bodyweight at the hip. At 94 kg, that is 235 to 330 kg of cyclic load through the construct, repeated 160 to 180 times per minute, for the duration of a run. A modest 40 km running week is on the order of one million loading cycles per year through the nail.
Ti6Al4V ELI under physiologic conditions has a fatigue endurance limit well above the loads a healed femur places on the implant once the bone is sharing the load. What this means in practice: an IM nail in a healed femur, in a normal-sized canal, is not the part of the system that limits the athletic career. The bone-implant interface, lag screw position, and bone density are higher on the failure-risk list than the nail itself.
The caveat for me specifically is the under-sizing my surgeon flagged. A nail with less canal contact and a body weight at the high end of the design envelope reduces the safety margin. It does not eliminate the margin. It does shape the conservatism of the first two years — no jumping, no plyometrics, no HYROX sled work before the bone has fully remodelled around the construct, no track sprinting in the rebuild.
Sport-by-sport hardware load
- Swimming: negligible femur load. The construct is mechanically idle in the pool. This is why the swim leg returns first.
- Cycling: closed-chain compressive loading at predictable angles, zero impact. Stationary cycling is one of the safest activities the construct experiences. Outdoor cycling adds the crash risk back, not the loading risk — which is exactly the right reason to be cautious in the aerobar progression next time around.
- Walking and easy running: moderate compressive loading well within fatigue tolerance once bone union is established. The bone-implant interface tolerates this comfortably after Month 6.
- Fast running and racing: higher peak loads at faster paces, particularly during the push-off phase. Carbon-plated racing shoes change the loading profile in ways the literature has not fully characterized yet. Worth watching, not worth fearing.
- HYROX stations: sled push and sled pull put substantial horizontal shear at the hip. Walking lunges and sandbag lunges load the operated leg through deep flexion. Burpee broad jumps create high-impact landing peaks. None of these are appropriate before the bone is fully remodelled, which is typically Month 12 to Month 18 post-op.
- Heavy strength training: back squats and deadlifts at meaningful loads compress the femur axially. Manageable once full weight bearing and gait normalization are complete. The first squat back under a bar is sometime in Month 4 to Month 5, at empty-bar loads, with the same progression I would prescribe to a beginner.
The implant is not the bottleneck. The bone-implant interface is.
The mode of failure I plan around is not the nail breaking. It is the lag screw migrating in the femoral head before callus has secured it in place, or the bone around the distal interlock screw fatiguing from premature loading. Both are early-stage failures that get designed out by following the surgeon's protocol through the first six months. After that, the construct settles into a load-sharing relationship with the bone, and the failure-risk curve flattens dramatically.
For an athlete planning a long career on this hardware, the practical operating rules are simple: respect the early protocol unconditionally, do not negotiate with the timeline based on how the leg feels, and keep the strength base broad enough that no single discipline asks too much of the operated side. The implant will outlast the rebuild.
What This Means If You Are in the Same Spot
If you have woken up after surgery for a similar fracture, here is what is worth doing in the first week:
- Get the implant card. A formal document with the manufacturer, model, material, lot number, and the surgeon's name. Most hospitals issue one at discharge. If yours does not, ask for one. Save a copy on your phone for MRI bookings, future surgeries, and airport security.
- Photograph your X-rays. A clear photograph of the post-operative AP and lateral films, with the date and time, becomes your reference image for every later visit. Hospital PACS systems are not always portable; your phone is.
- Get the operative note. The written record of what the surgeon did is your single most important piece of documentation. Lag screw position, distal interlock pattern (static vs dynamic), reduction technique, intraoperative findings. Request a copy in writing.
- Know your fracture type by name. Not just "broken femur." AO/OTA classification (31A1, 31A2, 31A3, 32A, 32B, 32C) determines the rehab path. Ask your surgeon to write it on the discharge summary.
- Build the timeline backwards from the next imaging. Your weight-bearing decision is made on a follow-up X-ray, not on how you feel. Mark the date on the calendar. Everything between now and then is gated on that image.
Where to Go Next
The day-by-day version of what this construct lets me do, week by week, lives in the broken femur recovery time timeline. The full first-person recovery log, with the medication stack and PT progression in one place, is the pillar page. The plan for the Ironman comeback that this hardware is designed to survive lives at Road to Roth 2027.
Frequently Asked Questions
What is a cephalomedullary nail?
A cephalomedullary nail is an intramedullary rod placed inside the femoral shaft with an additional screw — the lag screw — that travels from the lateral side of the femur, through the nail itself, and up into the femoral neck and head. The "cephalo" part refers to the cephalic (head-end) screw. This construct is designed for fractures in the proximal femur — intertrochanteric, subtrochanteric — where load must be transferred from the femoral head, around the fracture, and into the shaft.
What is the difference between PFN, PFNA, and TFN intramedullary nails?
PFN (Proximal Femoral Nail), PFNA (Proximal Femoral Nail Antirotation), and TFN (Trochanteric Fixation Nail) are all variants of the cephalomedullary nail family from different manufacturers. PFN typically uses two screws in the femoral neck (a lag screw plus an antirotation screw). PFNA uses a single helical blade instead of two screws — designed to compress osteoporotic bone rather than cut through it. TFN is a Synthes-branded variant with similar geometry. Mine is a Mediox PFN with a single cephalic lag screw — the original two-screw construct, simplified.
What does "Ti6Al4V ELI" mean?
Ti6Al4V is the most common medical-grade titanium alloy — titanium with 6% aluminum and 4% vanadium by weight, giving it the strength and biocompatibility profile that orthopaedic surgeons rely on. ELI stands for Extra Low Interstitial, a specification under ASTM F136 that limits oxygen, nitrogen, and iron content in the alloy. This matters because lower interstitials translate into better fatigue resistance under cyclic load — exactly what an implant carrying a 94 kg athlete needs.
Is a titanium femur nail MRI safe?
Modern titanium intramedullary nails are non-ferromagnetic, which means they do not move or heat dangerously in an MRI scanner. They are classified as MRI-conditional, not MRI-safe — the distinction matters. At 1.5T and 3T field strengths with standard sequences and SAR limits, the implant is safe to scan. At higher fields, or with high-SAR sequences, the manufacturer's specific MR conditions document must be consulted. For images of the femur or hip directly, MARS (Metal Artefact Reduction Sequences) should be requested.
What is the calcar femorale and why does it matter?
The calcar femorale is the dense medial cortical bone that runs from the lesser trochanter up the inside of the femoral neck. It is the natural compressive buttress that transfers load from the femoral head into the shaft when you stand. When the calcar is fractured or comminuted — as in my injury — the natural load path is broken. Until callus bridges that gap, the implant alone bears the compressive load. Early loading on a disrupted calcar risks varus collapse (the head tilts inward), lag-screw cut-out through the femoral head, or fatigue at the nail itself.
Why use an intramedullary nail instead of a plate for a subtrochanteric fracture?
For subtrochanteric and intertrochanteric fractures, an IM nail is biomechanically superior in two ways. First, it sits centrally inside the bone, so the load path runs through the nail rather than off-axis through a side-mounted plate — this dramatically reduces bending moments on the implant. Second, the IM nail load-shares with the bone as healing progresses: the bone gradually takes more compression as callus matures. A laterally placed plate continues to load-bear in isolation, which is one reason plates have higher failure rates in this fracture zone. The exception is fracture patterns extending too far distally for an IM nail to capture, where a plate becomes necessary.
Do you need to take the rod out after a femur fracture?
Generally, no. Modern titanium IM nails are designed to stay in the body indefinitely. Removal is indicated only if the hardware causes pain, soft-tissue irritation, prominent trochanteric tip, or rare hardware-related complications. For active patients returning to sport, leaving the nail in place is the default. My implant card explicitly notes "hardware removal not planned — earliest 2028." Removal becomes more nuanced if you plan a hip replacement decades down the line, but that decision belongs to that future surgeon.
How long does the surgery itself take?
For a closed reduction with an intramedullary nail in a subtrochanteric pattern, theatre time is typically 60–90 minutes once the patient is positioned and prepped. The operative steps are: closed reduction on a fracture table under fluoroscopy, lateral skin incision near the greater trochanter for the nail entry, antegrade insertion of the nail down the canal, fluoroscopic confirmation of position, drilling and placement of the cephalic lag screw, drilling and placement of the distal interlocking screw, end cap, closure. Most of the operative time is spent on positioning, reduction, and intraoperative imaging — not on cutting.
Ready to Train Smarter?
Get personalized training zones, race predictions, and performance insights with our free calculators.