

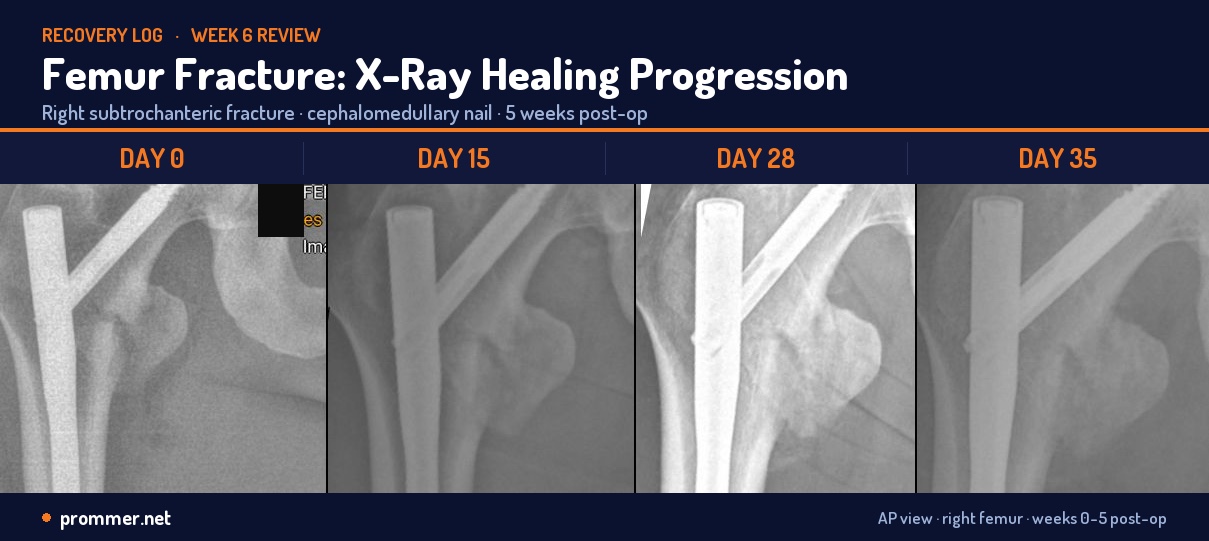
How long is the recovery time for a broken femur? A broken femur takes 12 to 16 weeks to reach clinical bone union in an adult with surgical fixation and 3 to 6 months to walk normally again, with running usually returning at Month 4 to 6. The femur surgery recovery timeline runs in gates, not dates — every step is cleared by an X-ray showing bridging callus, not by the calendar. Below is my own week-by-week broken femur recovery timeline from a comminuted subtrochanteric fracture, updated as each milestone lands.
This is the real timeline from my own recovery, drawn from a daily log I started in the hospital. The detail runs day by day through the first three weeks, then milestone by milestone to Week 8 (mid-June 2026): the non-weight-bearing wait, the Week 6 X-ray that cleared partial weight-bearing, and where the gait actually is now. Everything past Week 8 is still the plan, not the result — I update this page as each milestone lands, or as the plan changes when it meets reality. Recovery from a comminuted subtrochanteric femur fracture is not on rails; it is on radiographs — the Week 6 film, not the calendar, is what cleared the load.
Overview at a Glance
| Phase | Window | Key goal | Status |
|---|---|---|---|
| Acute / inpatient | Day 0–7 | Surgery, pain control, DVT prophylaxis, discharge | Completed |
| Early home recovery | Day 7–14 | NWB gait, home PT, supplement stack online | Completed |
| Suture removal & renewal Rx | Day 14–28 | Week 2 X-ray, new pain plan, accelerated PT | In progress |
| Pre-partial-weight-bearing | Day 28–42 | Active ROM, hip abduction, standing prep | Upcoming |
| Weight-bearing progression | Week 6–12 | Cleared to 50% at Week 6 → 100% over Weeks 6–8 | Confirmed June 3, 2026 (bridging callus) |
| Gait normalization | Week 12–16 | Single-crutch transition, normal walking | In progress — July 13 review cleared full activity (walking, swim, bike) |
| Return to running | Month 4–6 | Walk-jog progression, gait quality the gate | Surgeon-projected light jog ~Week 16 (mid-Aug 2026) |
| Ironman build | Month 6–14 | Swim → bike → run, periodized to Roth 2027 | Planned, target July 4, 2027 |
Days 0 to 7: The Hospital Week
Day 0 (Tuesday, April 21, 2026)
Crash on the first outdoor ride with aerobars at 15:00 ICT. Right subtrochanteric femur fracture. Pre-operative imaging at the small local clinic, then escalation to BVDK Tâm Anh, Tân Bình. Surgery began the same evening. Cephalomedullary intramedullary nail, cephalic lag screw, distal interlock, end cap. On the operating table by ~23:00, eight hours door-to-door. Same-day surgery is one of the strongest single determinants of outcome for this injury. Earlier fixation reduces soft-tissue swelling and infection risk and allows earlier mobilization.
Day 1 to Day 3: bed-based
Positioning every two hours, half-lying or Fowler's, then progressively more upright with pillows. Ankle pumps 25 reps twice a day for DVT prophylaxis. Ultracet and Celecoxib for pain. Rivaroxaban 10 mg once daily for anticoagulation. Cefuroxim for infection prophylaxis. Gabapentin at night. No weight bearing, no hip flexion past 0°, no hip abduction. ROM target for this window is hip flexion 0–20°, knee flexion 0–30° by Day 5.
Day 4 to Day 6: first ROM work
Passive range-of-motion work in supine with the hospital PT. Isometric quadriceps, glute, and hamstring sets: squeeze the muscle without moving the joint. Cryotherapy on the surgical sites. Continued ankle pumps. ROM target by Day 8 is hip flexion 0–30°, hip abduction 0–15°, knee flexion 0–45°. The hospital extended the stay through Tuesday to make sure transfers and bathroom logistics were sorted before discharge. That was the right call. The first week home breaks a lot of people who go home too early.
Day 7 (Monday, April 28): Discharge Day
Discharge from BVDK Tâm Anh. NWB for 4 more weeks confirmed by BS Lưu. Discharge prescription locked in: Cefuroxim, Celecoxib, Ultracet, Esomeprazole, Rivaroxaban, Gabapentin (all on a 7-day course). An Pháp PT home visit at 18:00, the first session at home. Iron labs come back normal (ferritin 151.4). Race deferrals submitted: Da Nang 70.3 medical deferral with surgeon's letter, Challenge Roth transfer to 2027.
Days 8 to 14: First Week Home
Day 8: First home day
Day 2 of 7-day prescription. Outreach to multiple clinics for outpatient PT (FV, CMI, JIO, Raffles, SPS, Maple, AIH). The orthopaedic clinic network in HCMC is highly variable. Some clinics do not do home visits, some do not have IM-nail-femur experience, some are happy to coordinate with BVDK Tâm Anh. The shortlist process took a week and is a separate rabbit hole.
Day 9: Ice pack arrives, new home-visit PT
Reusable gel ice pack added to the post-PT routine, 15–20 minutes wrapped in cloth, never directly on skin. New home-visit PT (referral from the BVDK Tâm Anh hospital PT) started at 16:00. More aggressive than the An Pháp session: passive-assisted right-leg straight-leg raise (could not lift unassisted), side-lying hip abduction from bed-edge as homework. Crutch gait corrected to a three-point NWB pattern: crutches and right (injured) leg advance together with no load, then the healthy left leg swings through with body weight on the crutches.
Day 11: First deep-tissue session with Vinh
First night sleeping in own bed instead of the hospital-rented bed. Only about 2 hours of actual sleep, but it felt better than the hospital bed in the morning. Vinh (Nhựt Vinh, hospital-referral PT) home visit at ~17:00. Different approach: deep-tissue massage along the right leg including the surgical area, more passive-assisted SLR work, lots of standing practice. Subjective comfort gain real, with no adverse reaction the next morning. Flagged at the Day 15 visit for explicit BS Lưu sign-off on deep tissue over the IM-nail entry.
Day 13: First PT-provoked pain
First time pain has been provoked by a PT session rather than eased by one. Second PT slot cancelled rather than push through. Pacing over pushing in Week 2. Day 7 of the prescription cycle: last doses of Cefuroxim, Ultracet, Celecoxib, Esomeprazole, Rivaroxaban, plus the final 7th gabapentin night.
Day 14: The NSAID-washout pain day
Significant pain day. Pain breakthrough at 3.5 hours on paracetamol monotherapy (1 g at 01:00, 1 g at 04:30), well inside the safe re-dose window, meaning paracetamol alone is not holding the pain. Pain sits in the expected NSAID-washout window: Celecoxib half-life is roughly 11 hours, so the anti-inflammatory effect clears 24–48 hours after the last dose. Day 13/14 PT-provoked residual stacks on top of that, plus unrelieved swelling driving mechanical pain. No fever, no drainage. The bridging analgesia question becomes the top ask for the Day 15 visit.
Days 15 to 21: Sutures Out, New Rx, First Real Progress
Day 15 (Tuesday, May 6): Week 2 visit with BS Lưu
The first follow-up since discharge. Vitals at intake: 94.0 kg, 196 cm, BMI 24.5, BP 148/90, HR 103. All flagged OK.
- Suture removal: very pain-free, quick. No bandage afterwards; air-healing protocol. Distilled-water clean as needed. No topical for 48 hours (Day 18 is the silicone scar-care kickoff).
- X-ray: hardware unchanged from Day 0, fracture appearance fine. Subtle haziness on the medial cortex consistent with very early periosteal callus initiation.
- Weight-bearing: NWB for 4 more weeks from today. Week 6 imaging on June 3 will decide whether 25% partial weight-bearing begins.
- Renewal Rx (14-day course, May 6 to May 19):
- Celecoxib 200 mg, 1 capsule AM + 1 capsule PM
- Ultracet (paracetamol 325 + tramadol 37.5), 1 tablet three times a day
- NextG Cal, 2 capsules AM (calcium hydroxyapatite + D3 + K1)
- Gabapentin (Neurontin) 300 mg, 1 capsule at night
- What is not in the new Rx: Rivaroxaban (operative DVT window closed), Esomeprazole (no GI symptoms on Celecoxib), Cefuroxim (course complete).
- Massage clearance: deep tissue including the surgical area cleared verbally.
- Other instructions: rest, elevate the leg, limit activity. Avoid low chairs, stairs, squatting, kneeling, cross-legged sitting, and leg-crossing.
Day 16: The Rx works
First full pain-zero day since the crash. 7.5 hours of largely unbroken sleep, the first night since surgery that pain has not dictated the sleep window. The renewal Rx is doing exactly what it was designed to do: Celecoxib for inflammation, Ultracet for breakthrough analgesia, Gabapentin for night-time neuropathic coverage. The 04:00 wake, 20:00 bed window is now empirically validated.
First day without a PT session since Day 7. A deliberate rest day. Wound cleaned with distilled water as instructed; open-air healing continuing.
Day 17: Barber day, two bad movements
First trip out for a non-medical reason since surgery: 11:00 barber appointment, six-seater Grab cab each way. Two accidental loading moments getting in and out of the chair. The NWB discipline that holds fine inside the apartment slips outside it when attention is on a non-walking task. Useful lesson for any future out-of-routine trip: brief the helper, set the chair height, plant the crutches deliberately, treat every transition as a high-risk movement window.
Day 18 (Saturday, May 9): First shower, silicone scar-care starts
48 hours past suture removal — the standard window for water contact after suture removal. First shower since surgery: short, lukewarm, no scrubbing the incision, pat dry, 10 minutes air-dry before any topical. Silicone scar-care protocol starts (Mepiform tape, cut to incision length, 12–24 hour wear, replaced every 2–3 days).
Two PT sessions in one day, the heaviest single-day mobility load yet: Billy (US-trained PT, Phan/Martin referral) at 10:00 for the first assessment session, then Vinh in the PM for continued Phase 2 work. EMS machine applied in Billy's session as priming. No red flags from either session.
Day 20 (Monday, May 11): First unassisted SLR
The first unassisted right-leg straight-leg raise. First time the operated leg has lifted under active hip-flexor control with no manual assist from a PT. The trajectory:
- Day 9: passive-assisted only, the leg dropped under its own weight
- Day 11: still passive-assisted, many reps with Vinh, no unassisted lift
- Day 20: unassisted. Nine days from passive-assisted introduction to active execution.
This is on schedule for a comminuted intertrochanteric / subtrochanteric pattern with calcar involvement and lesser-trochanter avulsion plus PFN fixation. The generic Week 2 target in the PT protocol assumes a stable A1 pattern or diaphyseal shaft fracture, which this is not. Literature for unstable 31A3-pattern fractures fixed with a PFN puts unassisted SLR commonly at Week 3–4 post-op. On schedule is the correct frame.
Two clinically meaningful sub-signals: the lesser-trochanter avulsion is not producing persistent iliopsoas dysfunction (active hip flexion against gravity would not be possible if iliopsoas were non-functional), and the hardware is stable enough to tolerate the shear load of unassisted hip flexion at Day 20.
Weeks 3 to 6: The Long Wait
This is the segment of recovery I am living in as this article goes live. The work is unglamorous: maintain the prescription cycle, hit PT four times a week, keep the supplement stack consistent, sleep eight hours, walk on crutches without loading the operated leg, accumulate strength on the contralateral side. The mood drop predicted by Week 2 to Week 4 is in the post. I will update the daily log honestly when it arrives.
- Week 3 ROM targets: hip flexion 0–70°, hip abduction 0–35°, knee flexion 0–90°. Add active hip abduction in side-lying.
- Week 4 ROM targets: hip flexion 0–90°, hip abduction 0–45°, knee flexion 0–110°. Standing-balance preparation on crutches, no weight bearing yet.
- Week 6 imaging (June 3, 2026): the decision-gating X-ray. Bridging callus on the medial cortex is the criterion for 25% partial weight-bearing.
Day 39 (Saturday, May 30): A fall, and a sprained wrist
The honest update the section above promised. Four days before the Week 6 X-ray, I fell — the first fall of this recovery. I went down on my left side and put my hand out. The operated right leg took some load in the fall, but it produced no new hip, incision, or hardware pain afterward, which is the part that matters most. The damage landed on the non-operated side: a sprained left wrist.
- Left wrist: same-day at American International Hospital — X-rayed (no fracture), diagnosed as a sprain, splinted. The cost of the urgent visit, consult, wrist X-ray and splint was 2,757,500 VND, roughly €100 / $108. For reference, the routine Day-28 follow-up with imaging was 1,950,000 VND.
- Operated right hip: no new pain, but a fall is exactly the event a comminuted fixation is told to avoid. It goes on the list for June 3 — I want the surgeon to look at the right-hip film and clear it specifically, not just read it for callus.
- Why a wrist sprain is not a footnote here: non-weight-bearing means the crutches carry the load, and the crutches load the wrists. A splinted left wrist degrades safe crutch mechanics at the worst possible moment — the highest fall-risk window of the recovery, right before the weight-bearing gate. The real risk of a sprained wrist in this situation is a second fall.
The "What Would Change This Plan" section below lists a re-injury during the rebuild as one of the three things that move the whole timeline. It showed up early — and it hit the wrist, not the femur, which is the version I will take. The protocol does not change: stay strictly non-weight-bearing on the right leg, do not let wrist pain tempt loading it, minimise out-of-house crutch trips until the wrist settles, and bring the whole episode to the June 3 appointment.
Week 6 (June 3): The X-ray cleared me — weight-bearing begins
The gate opened. The June 3 film showed initial bridging callus on the medial cortex — the exact criterion the whole non-weight-bearing phase had been waiting on. The surgeon also read the right-hip film specifically after the Day-39 fall and cleared it: no new damage to the fixation. With both boxes ticked, I went from strict non-weight-bearing straight to 50% partial weight-bearing, with instructions to build from 50% to full (100%) over the next two weeks on two crutches, then keep the crutches for roughly two weeks after reaching full load. A faster ramp than the conservative 25%-first plan I had written down — the callus earned it.
Week 8 (mid-June): Single crutch, but the gait isn't back
Two weeks into the load progression, and the picture is honest. I am walking more and more freely and now get around outside on a single crutch instead of two. The hard part: my gait is still very off, and walking on a fully extended leg is still challenging and genuinely painful. Standing fully on the operated leg with the knee locked out, it can still feel like it might give way — I am not yet confident it holds 100%, and a single-leg hold maxes out around 15 shaking seconds before the deep pain comes on if I let the weight off too quickly. "Cleared to weight-bear" is not the same as walking normally — the leg holds the load, but the mechanics and the pain have a long way to go.
- Pain management: off all painkillers since the end of Week 4 — the wean itself was a non-event. The genuinely hard pain stretch came earlier, a single day at the Week 2 mark with a gap in cover (the NSAID-washout day), when pain broke through paracetamol in 3.5 hours and forced the renewal prescription. The stack is supplements only now — calcium and vitamin D at doses sufficient for bone healing, alongside the rest of the recovery stack.
- Back in the water: first real swim this week — straight-line freestyle, a few 50 m lanes, gentle kick only (breaststroke's whip kick is still off-limits). The pool is the first place the leg moves at full range without carrying body weight, and walking the water (forward, backward, sideways, on toes and heels) is the cleanest gait practice I have. The real hazard in a public lane is another swimmer kicking the leg, not the swimming itself.
- Strength: more floor work and targeted strength training over the last two weeks, rebuilding the operated side at light loads as the bone takes more.
- GLP-1, back on: I stayed off tirzepatide from surgery onward so I could eat enough to heal the bone — weight drifted from about 93 kg up to roughly 96 kg. With the leg loading now, I restarted at maintenance in early June and I'm back to just under 94 kg. Full arc in the GLP-1 June update.
Week 10 (late June): The leg starts holding a straight knee, and the cardio engine comes back
The single change I was waiting for has started to land: I can now walk on a single crutch with the operated leg fully extended through stance, cleanly, without the knee feeling like it will give way. At Week 8 a locked-out leg under load still "broke away" — the quad and glute were not recruiting fast enough to trust the straight-knee position. That is the deficit that is now closing. The gait is not normal yet, but straight-knee load tolerance is the prerequisite for normal, and it is arriving.
Two things are doing the most work for it: loaded stretching and standing cable rows on the operated leg, plus the single-crutch walking itself with the knee held straight. Cable rows read as a back exercise, and they are — but done standing they force the operated leg to stabilise under a pulling load through a fully extended knee, which is the pattern stance needs.
- First real sweat: my first proper spin session — the first time since the crash that a cardio effort was hard enough to actually break a sweat, not just turn the legs over. The bike is seated, so the healing leg never carries the body-weight column that standing and walking drive through it, and pedaling loads the femur at a fraction of walking — the bone stays lightly loaded even when the effort runs high. That is why it is the safest place to reopen real conditioning. The session is logged here. The group I have to keep honest is the adductors and side hip — resisted riding on consecutive days aggravated them earlier in the month, so spin stays every second day.
- Breaststroke is back on the table. At Week 8 I wrote that breaststroke was off-limits because the whip kick loads the hip in abduction and external rotation — the contraindicated plane. By late June, both freestyle and breaststroke felt OK for the first time. Breaststroke still causes more discomfort than freestyle, which is exactly what the mechanics predict, so it stays gentle and gets a check with the PT before I load it harder. Freestyle with a light kick is the workhorse; breaststroke is something I test, not train.
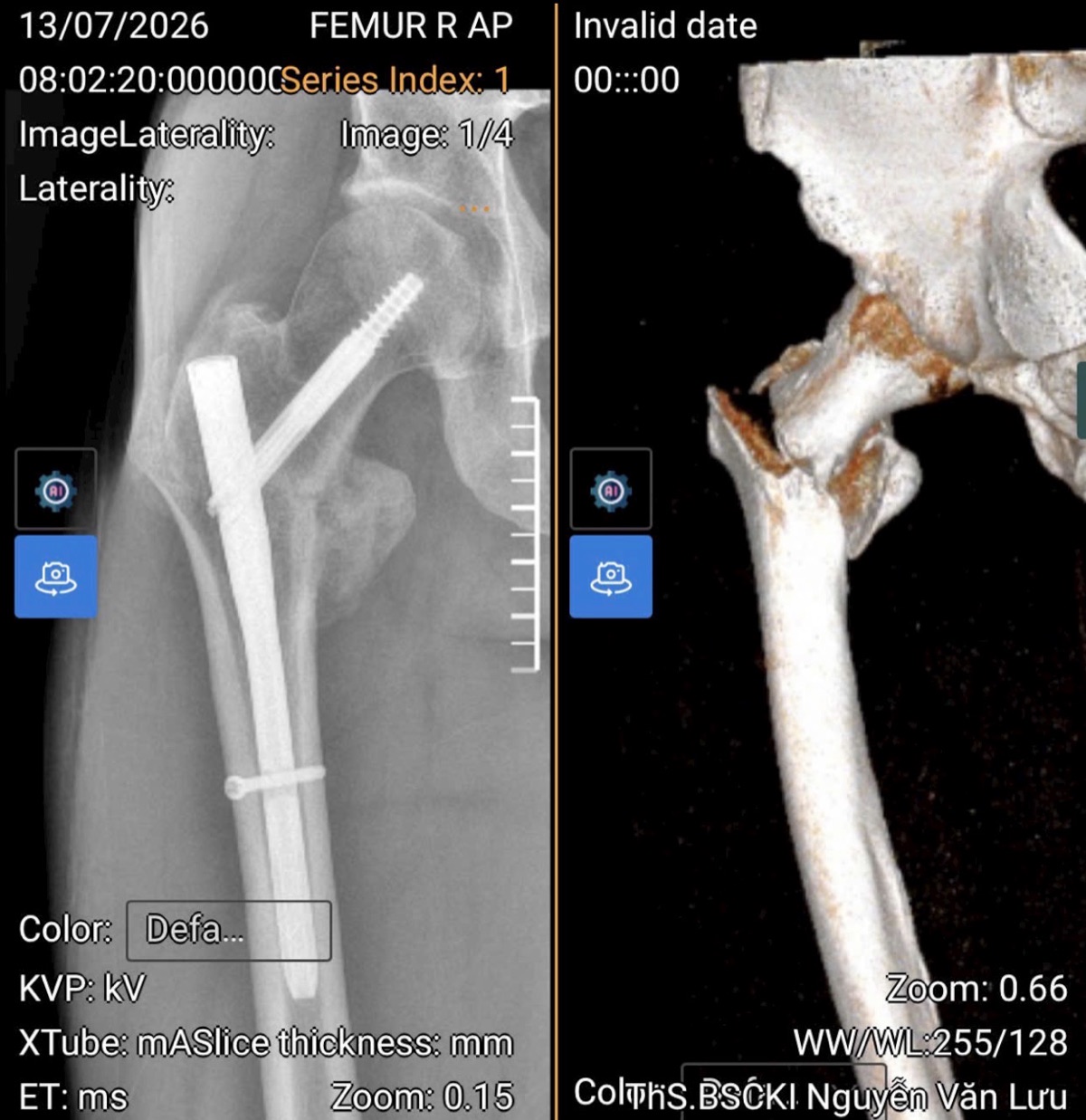
Week 12 (July 13): The surgeon clears full activity — and the jog gets a date
The Week 12 review with BS Lưu, the gate I had been walking toward. New films — both hips AP plus the right femur AP and lateral — and the read was the word you want at twelve weeks: healing is on par, right where the construct should be. On the strength of that he cleared me for full activity: swimming, biking, and longer walks, and finally put a date on the milestone this whole page is written toward — light jogging in about four weeks, which lands at Week 16. That is not the timeline slipping; it is the conservative Week-16 walk-jog window I had penciled in, now confirmed by the surgeon reading the actual X-ray instead of guessed from a textbook.
- The hardware stays. I asked about taking the nail out. His answer: leave it. The nail does not protrude, so removing it would be technically difficult and risks damaging the bone on the way out — a poor trade against a construct that is doing its job. Nail removal is back on the table only if it ever starts to hurt. For an athlete that is the right call: an elective second surgery on a healed femur buys nothing but downside.
- Calcium comes off the stack. With union tracking on schedule, the supplemental calcium is no longer required — twelve weeks of bone-healing support did its job, and the stack gets lighter.
- What "cleared" actually unlocks. Not intensity — load. The clearance is permission to put the operated leg under real, progressive weight-bearing work: longer walks, loaded carries, the bike without hedging. The jog is still four weeks out because impact is its own gate, separate from bone union.
- No added-weight leg exercises yet. The one thing he did not sign off on: adding external load to leg-strength work. Loaded carries and the ruck walk are fine — that is axial load through a healing bone doing what walking already does — but weighted squats, leg press, or any added-resistance single-leg work stay off the table until he clears them. Leg strength stays bodyweight for now; the upper body and the healthy side load normally.
And the training log finally reads like training again. Walking is the new centerpiece: a first 30-minute walk on Saturday, July 11 (2.9 km, HR 110) that felt genuinely okay, then a 40-minute walk on Monday the 13th carrying a 10 kg backpack (3.9 km) — deliberately loading the leg through a long, low-impact effort now that the surgeon has signed off on exactly that. The spin classes are back too: a 50-minute indoor session on the 12th at an average 162 bpm (256 TSS) — a real sweat effort, not a gentle turnover — with strength work the same day. Seated cycling still carries the heavy conditioning because it pedals the femur at a fraction of walking's load, but the story of Week 12 is that walking, the thing that actually loads the healing bone, went from careful steps to a loaded ruck in the space of a weekend.

Weeks 6 to 12: Progressive Weight Bearing
The June 3 X-ray confirmed the bridging callus, so this phase is now live — on a faster ramp than the conservative version below (50% from Week 6 rather than 25%). The milestone structure still holds:
- Week 6 to Week 7: 25% partial weight-bearing on the operated leg. Gait re-education on two crutches with consciously loaded steps. Pool work cleared if wounds are fully sealed.
- Week 7 to Week 8: 50% partial weight-bearing. Pool work continues, stationary cycling with low resistance begins. Single-leg dumbbell work on the operated side becomes possible at very light loads.
- Week 9 to Week 10: 75% partial weight-bearing. Functional ROM near full. Step-ups onto a low box with the operated leg start as a strength reintroduction movement.
- Week 10 to Week 12: 100% weight-bearing on two crutches, transition to single crutch, gait normalization. Stationary cycling moves to moderate resistance. Walk-jog intervals not yet. Bone first.
The contingency I had written for — no callus at Week 6, non-weight-bearing extended another 2–4 weeks — did not come to pass. The callus was there on June 3 and the ramp began on schedule. The X-ray decided, not the calendar.
Weeks 12 to 24: Return to Walking, Then Running
- Week 12 to Week 16: crutch-free walking. Normal gait, no limp, hip flexor and glute strength on the operated leg restored to within 15% of the contralateral side.
- Week 16 to Week 20: walk-jog intervals. Short jogging bouts (30 seconds to a minute) on soft surface, with walking recoveries. The operated leg must absorb the impact load without pain, swelling, or compensation in the gait.
- Week 20 to Week 24: continuous easy running. Time on feet, not pace. Easy aerobic running 20–40 minutes, three to four times a week. Single-leg strength benchmarks at 80%+ of the contralateral side before any structured running.
Month 6 to Month 14: The Ironman Build
The full periodization plan to Challenge Roth 2027 lives in the Road to Roth 2027 article. The short shape:
- Month 6 to Month 8: aerobic base rebuild across the three disciplines. Swim engine first (already largely recovered by this point), bike second, run third. Volume over intensity.
- Month 8 to Month 11: threshold work. Tempo runs, sweet-spot bike intervals, threshold swim sets. Build run mileage to 60–70% of pre-crash peak.
- Month 11 to Month 13: Ironman-specific build. Long brick sessions, race-pace bike volume, marathon-pace tempo runs. A B-race for confidence (likely a half-Ironman in late Q1 2027).
- Month 13 to Month 14: taper and race. Challenge Roth 2027, Sunday July 4, 2027.
Athletic Metrics Through the Recovery
A separate read of the same timeline, this time through the lens of fitness rather than orthopaedic milestones. These are the numbers I will be tracking as benchmarks of the comeback, not just whether the bone heals.
Baseline before the crash (December 2025)
- Body composition: 94.0 kg, 196 cm, ~11% body fat, 83 kg lean mass.
- Cycling FTP: 261 W, 2.77 W/kg. Targeting 280 W (3.0 W/kg) by Roth 2026.
- Run thresholds: LT1 at 7:05/km @ 140 bpm, LT2 at 5:10/km @ 166 bpm. Max HR 190.
- Marathon prediction: 3:49 (Garmin), targeting 3:45–3:50 in real conditions.
- Resting HR: 59–63 bpm, the lowest end of an active 46-year-old male range.
Detraining curves I expect
- VO2max: 5–10% loss per month of complete inactivity, gradually slowing. Realistic floor at Month 3 is roughly 80% of pre-crash. Lower-body strength loss is steeper than aerobic loss.
- Cycling FTP: typically 5–10% per month, but cycling has the best contralateral and aerobic carry-over of the three disciplines. With swim engine running and contralateral leg work loaded heavily, expect FTP at Month 3 to be 220–240 W rather than the textbook 200 W.
- Run economy: the slowest to come back. Specific running fitness needs running, and running is gated on bone healing. Realistic LT2 pace at first run-clearance (Month 4–5) is somewhere around 5:30–5:40/km at the same heart rate, with weeks of progression needed to approach pre-crash thresholds.
- Swim CSS: swim-specific fitness is the most preservable. With pool work starting Week 4–6 and full sessions by Month 2, expect CSS to be within 5% of pre-crash by Month 4 and back to baseline before the run engine is even cleared.
- Lean mass: the surprising one. Even with aggressive contralateral loading and high protein intake, 4–6 kg of estimated lean mass loss across the first 3 months is realistic. The GLP-1 cluster on this site documents the same pattern from a different cause; the principle is the same — protein, resistance, and high training volume can slow muscle loss but rarely prevent it during a forced rest.
Re-entry milestones — what gets logged
- First pool session: aiming for Week 4 to Week 6. Pull-only, float between knees. The first 1,000 m back in the water gets a real entry in the daily log.
- First stationary bike session: conditional on Week 6 X-ray. 20 minutes, low resistance, just spinning. Heart rate, RPE, any pain — all recorded.
- First outdoor walk over 1 km: after full weight-bearing clearance (Week 10–12). Treated as a real session, not a chore.
- First easy jog: Month 4 to Month 5. 30 seconds, on a treadmill or track. This is the milestone I am writing toward.
- First continuous 5 km run: Month 5 to Month 6. The marker that says the run engine is rebuilding, not just starting up.
- First long ride over 60 km: Month 5 to Month 6. The Ironman bike volume rebuild begins here.
- First brick session: Month 8 to Month 9. Bike followed by a short run, the discipline-stack test that the Ironman build is actually possible.
- First half-Ironman: Q1–Q2 2027. The tune-up race ahead of Roth 2027. A fitness check, not a result.
- Challenge Roth 2027: Sunday, July 4, 2027. The line.
What the daily log captures that a clinical chart does not
- Mood through forced rest. Athletes lose identity faster than they lose fitness. The Week 2 to Week 4 mood drop is real and predictable. Three consecutive days under 5/10 is a coach call, not a "wait and see."
- Sleep quality independent of total hours. Seven hours of broken sleep is not seven hours of sleep. The Day-16 night that broke through pain (7.5 hours largely unbroken) was a different kind of recovery from the Day-14 night of pain breakthrough on paracetamol monotherapy.
- Subjective fitness perception. Athletes are unreliable narrators on their own recovery early on. Recording perceived fitness next to objective milestones forces honesty about the gap.
What Would Change This Plan
Three things could move the entire timeline:
- Delayed union or non-union at the Week 6 or Week 12 X-ray. If callus is not bridging on schedule, the weight-bearing progression slows and the running window pushes out. Worst case, a revision operation. This is the largest single risk in months 1 to 4.
- Hardware-related complications. Lag-screw migration, varus collapse, peri-implant fracture. Any of these resets the protocol.
- A re-injury during the rebuild. Stress reaction in the operated leg during the return-to-running phase, or a soft-tissue injury during the contralateral-loading work. Catching it early (the daily log exists for this) keeps it from becoming a season-ender.
None of these are likely if the protocol holds. All of them are possible if it does not.
Update Cadence
This page is updated as milestones land: Week 6 X-ray, first weight-bearing step, first shower, first pool session, first run. Last updated 2026-07-14. If you are reading this several months after that date and the page looks identical, the likely answer is that the next milestone slipped and the pillar page will have the explanation.
Frequently Asked Questions
How long does a broken femur take to heal in an adult?
Clinical bone union typically takes 12–16 weeks for an adult with surgical fixation, with remodelling continuing for 6–12 months. For comminuted patterns with calcar involvement (mine), the conservative trajectory is non-weight-bearing through Week 6, partial weight bearing Weeks 6–12, full weight bearing by Week 12–16, and return to running from Month 4–6 onward. Return to running and racing is a separate timeline from bone-union timing.
What does the femur surgery recovery timeline look like week by week?
The femur surgery recovery timeline runs in gates, not fixed dates. In my case: Day 0 same-day surgery; Week 1 discharge and home PT; Week 2 sutures out and first X-ray; Weeks 2–6 non-weight-bearing on two crutches; Week 6 the X-ray shows bridging callus and clears partial weight-bearing; Weeks 6–8 ramp from 50% to full load and transition to a single crutch; Week 8 first outdoor single-crutch walking; Week 10 straight-knee load tolerance and the cardio engine reopening; Week 12 the surgeon clears full activity — swimming, biking, longer walks — with light jogging projected around Week 16. Each unlock is decided by the radiograph, not by the calendar.
How long is the recovery time for a shattered or comminuted femur fracture?
A comminuted (shattered, multi-fragment) femur fracture recovers more slowly than a clean transverse break because the bone has to bridge several fragments before it can bear load. Bone union still lands in the 12–16 week range with intramedullary nail fixation, but the weight-bearing progression is more conservative: non-weight-bearing for roughly the first 6 weeks, partial weight-bearing gated on radiographic bridging callus, and full weight-bearing by Week 12–16. My own fracture was a comminuted AO 31A2/A3 subtrochanteric pattern with calcar involvement, and it followed exactly this conservative arc — the callus on the Week 6 film, not the calendar, is what cleared the load.
What is the recovery time for a broken femur fixed with a rod (intramedullary nail)?
A rod — an intramedullary nail — is a load-sharing implant, so it often allows earlier weight-bearing than a plate, but the recovery time still tracks bone healing: 12–16 weeks to union and 3–6 months to normal walking. Stable shaft patterns with a rigid nail can weight-bear within days; complex patterns like mine stay non-weight-bearing until the Week 6 X-ray confirms callus. The nail usually stays in permanently and is only removed if it later becomes painful — at my Week 12 review the surgeon left it in place because the construct was doing its job and removal on a healed femur carries more downside than benefit.
When can you put weight on a broken femur with a rod?
It depends on the fracture pattern, the hardware, and your surgeon. Stable fracture patterns with a rigid IM nail often allow weight bearing as tolerated within days. Comminuted patterns with calcar disruption typically stay non-weight-bearing for 4–6 weeks, with partial weight-bearing gated on radiographic bridging callus. My protocol was non-weight-bearing for 6 weeks; the Week 6 X-ray (June 3, 2026) showed bridging callus on the medial cortex and cleared me from non-weight-bearing straight to 50% partial weight-bearing, ramping to full over the following two weeks.
How long are you on crutches after a femur fracture?
For my conservative protocol, three-point non-weight-bearing gait on two crutches for 6 weeks, then progressive partial weight bearing on two crutches for another 6 weeks, then a single-crutch transition. Textbooks place that transition around Week 10–12; with a clean Week 6 callus I reached single-crutch outdoor walking at Week 8. Full crutch-free walking typically arrives between Week 12 and Week 16. Faster protocols exist for stable patterns; conservative protocols exist for more complex ones. The crutches stay until your surgeon and PT both clear them.
How long until I can walk normally again?
Normal gait — without crutches, without a limp, with balanced hip-flexor and glute strength — typically returns 3–6 months post-surgery. Walking is not the same as running, and running is not the same as racing. Each transition has its own clearance gate (radiographic union, full weight bearing, normal single-leg balance, restored single-leg strength, no pain on impact loading).
How long until I can run again?
For my fracture pattern and conservative protocol, the realistic return-to-running window is Month 4–6 post-surgery. Earlier in stable shaft fractures with rigid IM nails; later in complex patterns or with hardware issues. The progression is walk → walk-jog intervals → continuous jogging → easy running → structured running — each step gated on the operated leg absorbing the load without pain, swelling, or compensation in gait.
How long until I can swim or bike?
Swimming with the legs immobilized (pull buoy between the knees, no kick) typically becomes possible at Week 4–6 once the wounds are fully sealed and the surgeon clears submersion. My own first real swim came at Week 8: straight-line freestyle with a gentle kick only — a hard kick still hurt, and breaststroke was off the table because the whip kick loads the hip and adductors directly. By Week 10 both freestyle and breaststroke felt OK for the first time, though breaststroke still causes more discomfort than freestyle and stays gentle, as the whip-kick mechanics predict. Stationary cycling (unloaded, gentle resistance) usually opens up around the same time; my first genuinely sweaty spin session came at Week 10 — seated cycling keeps the body-weight load off the healing leg and pedals the femur at a fraction of the force walking puts through it, so the effort can run high while the bone load stays low. Outdoor cycling depends on bone union, balance, and crash risk — typically much later, often after Month 3–4. The swim engine and bike engine carry most of the early fitness work during the running drought.
Ready to Train Smarter?
Get personalized training zones, race predictions, and performance insights with our free calculators.